WO2005007166A1 - Treatment of sexual dysfunction - Google Patents
Treatment of sexual dysfunction Download PDFInfo
- Publication number
- WO2005007166A1 WO2005007166A1 PCT/IB2004/002286 IB2004002286W WO2005007166A1 WO 2005007166 A1 WO2005007166 A1 WO 2005007166A1 IB 2004002286 W IB2004002286 W IB 2004002286W WO 2005007166 A1 WO2005007166 A1 WO 2005007166A1
- Authority
- WO
- WIPO (PCT)
- Prior art keywords
- sexual
- methyl
- pyrimidin
- pyrazolo
- hsdd
- Prior art date
Links
Classifications
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K45/00—Medicinal preparations containing active ingredients not provided for in groups A61K31/00 - A61K41/00
- A61K45/06—Mixtures of active ingredients without chemical characterisation, e.g. antiphlogistics and cardiaca
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/495—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with two or more nitrogen atoms as the only ring heteroatoms, e.g. piperazine or tetrazines
- A61K31/496—Non-condensed piperazines containing further heterocyclic rings, e.g. rifampin, thiothixene
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/33—Heterocyclic compounds
- A61K31/395—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins
- A61K31/495—Heterocyclic compounds having nitrogen as a ring hetero atom, e.g. guanethidine or rifamycins having six-membered rings with two or more nitrogen atoms as the only ring heteroatoms, e.g. piperazine or tetrazines
- A61K31/505—Pyrimidines; Hydrogenated pyrimidines, e.g. trimethoprim
- A61K31/519—Pyrimidines; Hydrogenated pyrimidines, e.g. trimethoprim ortho- or peri-condensed with heterocyclic rings
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61K—PREPARATIONS FOR MEDICAL, DENTAL OR TOILETRY PURPOSES
- A61K31/00—Medicinal preparations containing organic active ingredients
- A61K31/63—Compounds containing para-N-benzenesulfonyl-N-groups, e.g. sulfanilamide, p-nitrobenzenesulfonyl hydrazide
- A61K31/635—Compounds containing para-N-benzenesulfonyl-N-groups, e.g. sulfanilamide, p-nitrobenzenesulfonyl hydrazide having a heterocyclic ring, e.g. sulfadiazine
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P15/00—Drugs for genital or sexual disorders; Contraceptives
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P15/00—Drugs for genital or sexual disorders; Contraceptives
- A61P15/08—Drugs for genital or sexual disorders; Contraceptives for gonadal disorders or for enhancing fertility, e.g. inducers of ovulation or of spermatogenesis
-
- A—HUMAN NECESSITIES
- A61—MEDICAL OR VETERINARY SCIENCE; HYGIENE
- A61P—SPECIFIC THERAPEUTIC ACTIVITY OF CHEMICAL COMPOUNDS OR MEDICINAL PREPARATIONS
- A61P15/00—Drugs for genital or sexual disorders; Contraceptives
- A61P15/10—Drugs for genital or sexual disorders; Contraceptives for impotence
Definitions
- This invention relates to the use of cyclic guanosine 3', 5'-monophosphate phosphodiesterase type five (PDE5) inhibitors, in combination with 5HT1a agonists for the treatment of sexual dysfunction, particularly female sexual arousal disorder (FSAD) with concomitant hypoactive sexual desire disorder (HSDD).
- PDE5 cyclic guanosine 3', 5'-monophosphate phosphodiesterase type five
- Male sexual dysfunction includes male erectile dysfunction, ejaculatory disorders such as premature ejaculation (PE), anorgasmia (inability to achieve orgasm) and desire disorders such as hypoactive sexual desire disorder (lack of interest in sex).
- PE premature ejaculation
- anorgasmia inability to achieve orgasm
- desire disorders such as hypoactive sexual desire disorder (lack of interest in sex).
- Desire or libido is the drive for sexual expression. Its manifestations often include sexual thoughts either when in the company of an interested partner or when exposed to other erotic stimuli.
- Arousal includes the vascular response to sexual stimulation, an important component of which is genital engorgement and increased vaginal lubrication, elongation of the vagina and increased genital sensation/sensitivity and a subjective excitement response.
- Orgasm is the release of sexual tension that has culminated during arousal.
- FSD occurs when a woman has an absent, inadequate or unsatisfactory response in any one or more of these phases, usually desire, arousal or orgasm.
- DSM-IV The American Psychiatric Association classifies female sexual dysfunction (FSD) into four classes: FSAD, hypoactive sexual desire disorder (HSDD), female orgasmic disorder (FOD), and sexual pain disorders (e.g. dyspareunia and vaginismus) [see the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV)]. DSM-IV defines the four classes as follows:
- FOD - Persistent or recurrent delay in, or absence of, orgasm following a normal sexual excitement phase Women exhibit wide variability in the type or intensity of stimulation that triggers orgasm. The diagnosis of FOD should be based on the clinician's judgement that the woman's orgasmic capacity is less than would be reasonable for her age, sexual experience, and the adequacy of the sexual stimulation she receives.
- Dyspareunia is the recurrent or persistent genital pain associated with sexual intercourse.
- Vaginismus is the recurrent or persistent involuntary spasm of the musculature of the outer third of the vagina that interferes with sexual intercourse.
- HSDD is the persistent or recurrent deficiency (or absence) of sexual fantasies/thoughts, and/or desire for or receptivity to sexual activity, which causes personal distress.
- FSAD is the persistent or recurrent inability to attain or maintain sufficient sexual excitement, causing personal distress, which may be expressed as a lack of subjective excitement, or genital (lubrication/swelling) or other somatic responses.
- FOD is the persistent or recurrent difficulty, delay in or absence of attaining orgasm following sufficient sexual stimulation and arousal, which causes personal distress.
- Dyspareunia is the recurrent or persistent genital pain associated with sexual intercourse.
- Vaginismus is the recurrent or persistent involuntary spasm of the musculature of the outer third of the vagina that interferes with vaginal penetration, which causes personal distress.
- HSDD is present if a woman has no or little desire to be sexual, and has no or few sexual thoughts or fantasies. This type of FSD can be caused by low testosterone levels, due either to natural menopause or to surgical menopause. Other causes in both pre-menopausal woman (i.e. woman who are pre-menopausal and who have not have hysterectomies) as well as post menopausal women include illness, medications, fatigue, depression and/or anxiety. Factors having a potential (conscious or sub-conscious) psychological impact such as relationship difficulties or religious factors may be related to the presence of / development of HSDD in females.
- FSAD is a highly prevalent sexual disorder affecting pre-, peri-, and post menopausal women. It is associated with concomitant disorders such as depression, cardiovascular diseases, diabetes and UG disorders. FSAD is characterised by inadequate genital response to sexual stimulation. The genitalia do not undergo the engorgement that characterises normal sexual arousal. The vaginal walls are poorly lubricated, so that intercourse is painful. Orgasms may be impeded. FSAD can be caused by reduced oestrogen at menopause or after childbirth and during lactation, as well as by illnesses, with vascular components such as diabetes and atherosclerosis. Other causes result from treatment with diuretics, antihistamines, antidepressants e.g. selective serotonin reuptake inhibitors or antihypertensive agents.
- Sexual pain disorders includes dyspareunia and vaginismus
- sexual pain disorders are characterised by pain resulting from penetration and sexual activity and may be caused by medications which reduce lubrication, endometriosis, pelvic inflammatory disease, inflammatory bowel disease or urinary tract problems.
- PDE5 inhibitors in combination with 5HT1a agonists work well in treating subjects who suffer from sexual dysfunction.
- the combination may be deemed synergistic.
- Suitable sexual dysfunctions include FSAD, HSDD and FOD in women and MED in men.
- the invention provides the use of a PDE5 inhibitor in combination with a 5HT1a agonist in the manufacture of a medicament for the treatment of sexual dysfunction
- the invention provides the use of a PDE5 inhibitor in combination with a 5HT1 a agonist in the manufacture of a medicament for the treatment of FSAD and HSDD in a subject suffering from FSAD and concurrent significant HSDD.
- significant HSDD means a level of HSDD which causes some degree of personal distress to the female subject.
- significant HSDD means a level of HSDD which causes some degree of distress and is measurable.
- the HSDD is measurable through evaluation by a clinician using a semi- structured questionnaire.
- More preferably significant HSDD means a level of HSDD which causes some degree of distress and is measurable as a score of less than or equal to 16 on the desire domain in the Sexual Function Questionaire (SFQ) hereinbelow.
- SFQ Sexual Function Questionaire
- a female subject with FSAD and significant HSDD may occasionally experience a slight increase in her desire, for example as a result of psychological factors. It will be appreciated that such a subject typically and generally has significant HSDD and is therefore included within the scope of the invention.
- concurrent means a subject who experiences FSAD at the same time as experiencing significant HSDD.
- concurrent does not encompass female subjects with situational HSDD, i.e. subjects who normally experience satisfactory levels of desire and who are normally able to become aroused, but occasionally are unable to experience any satisfactory levels of desire and arousal as a result of external factors, for example partner specific HSDD.
- the female subject is oestrogen and androgen replete.
- Replete levels of the oestrogen and androgen may already exist in the subject or they may be achieved artificially.
- Replete levels or oestrogen may be achieved artificially by administration of estradiol, estrone, estriol, a synthetic oestrogen (for example oestrogen benzoate), an agent which causes the body to produce oestrogen and/or an oestrogen receptor modulator/agonist (for example raloxifene or lasofoxifene).
- Replete levels of androgen may be achieved by administration of an androgen (such as include androsterone, dehydro- androsterone, testosterone, androstanedione or a synthetic androgen), an agent which causes the body to produce androgen and/or androgen receptor modulator/agonist (for example tibolone)
- an androgen such as include androsterone, dehydro- androsterone, testosterone, androstanedione or a synthetic androgen
- an agent which causes the body to produce androgen and/or androgen receptor modulator/agonist for example tibolone
- the term replete means having concentrations of oestrogen and androgen equal to or greater than minimum physiological concentrations found in a normal subject.
- Oestrogen is the general term for any substance having the physiological activity of oestradiol. It includes natural and synthetic oestrogens. Naturally occurring oestrogens include oestradiol, oestrone, oestriol and their conjugates, predominantly protein-bound. An example of a synthetic oestrogen is oestradiol benzoate. In a preferred embodiment the subject has a concentration of oestrogen equal to or greater than 40 picogrammes per millilitre of blood.
- Oestradiol concentration provides a reliable measure of total oestrogen levels in the body.
- the physiological concentration of oestradiol varies depending on the stage of ovulation.
- the minimum concentration of oestradiol (protein-bound and free) in a normal women is approximately 40 picogrammes per millilitre of blood. Therefore in a preferred embodiment the subject has a concentration of oestradiol (protein-bound and free) equal to or greater than 40 picogrammes per millilitre of blood.
- Coat-a-Count® Esradiol [available through DPC®(Diagnostic Products Corporation, 5700 West 96th Street, Los Angeles, CA900456-5597] provides a kit to measure the concentration of protein-bound and free oestradiol.
- Androgen is the collective term for a group of steroids, both natural and artificial. In females androgens are produced by the ovaries and adrenocortex. The natural androgens include androsterone, dehydro-androsterone, testosterone and androstanedione. Testosterone is by far the most potent natural hormone.
- the female subject can be pre-menopausal, peri-menopausal, post-menopausal or surgically menopausal i.e. post-hysterectomy. In a preferred embodiment the subject is post-menopausal.
- the PDE5 inhibitor means the PDE5 inhibitors for use with the invention.
- the term includes pharmaceutically acceptable salts, solvates and polymorphs of the PDE5 inhibitors for use with the invention.
- the suitability of the PDE5 inhibitor can be readily determined by evaluation of its potency and selectivity using literature methods followed by evaluation of its toxicity, absorption, metabolism, pharmacokinetics, etc in accordance with standard pharmaceutical practice.
- the PDE5 inhibitors have an IC50 against the PDE5 enzyme of less than 100 nanomolar, more preferably, at less than 50 nanomolar.
- IC50 values for the PDE5 inhibitors may be determined using the PDE5 assay in the Test Methods Section hereinafter.
- the PDE5 inhibitors are selective for the PDE5 enzyme. Preferably they have a selectivity of PDE5 over PDE3 of greater than 100 more preferably greater than 300. More preferably the PDE5 has a selectivity over both PDE3 and PDE4 of greater than 100, more preferably greater than 300.
- IC50 values for the PDE3 and PDE4 enzyme may be determined using established literature methodology, see S A Ballard et al, Journal of Urology, 1998, vol. 159, pages 2164- 2171.
- the PDE5 inhibitors have an IC50 against PDE5 of less than 100 nM and a selectivity over PDE3 of greater than 100 fold.
- PDE5 inhibitors for use with the invention are:
- Preferred PDE5 inhibitors for use with the invention are:
- (+)-3-ethyl-5-[5-(4-ethylpiperazin-1-ylsulphonyl)-2-(2-methoxy-1(R)- methylethoxy)pyridin-3-yl]-2-methyl-2,6-dihydro-7H-pyrazolo[4,3-d]pyrimidin-7-one also known as 3-ethyl-5- ⁇ 5-[4-ethylpiperazin-1-ylsulphonyl]-2-([(1 R)-2-methoxy-1- methylethyl]oxy)pyridin-3-yl ⁇ -2-methyl-2,6-dihydro-7H-pyrazolo[4,3-d] pyrimidin-7- one (see WO99/54333);
- Still further PDE5 inhibitors for use with the invention include: 4-bromo-5- (pyridylmethylamino)-6-[3-(4-chlorophenyl)-propoxy]-3(2H)pyridazinone; 1-[4-[(1 ,3- benzodioxol-5- ylmethyl)amiono]-6-chloro-2-quinozolinyl]-4-piperidine-carboxylic acid, monosodium salt; (+)-cis-5,6a, 7,9,9, 9a-hexahydro-2-[4-(trifluoromethyl)- phenylmethyl-5-methyl-cyclopent-4,5]imidazo[2,1 -b]purin-4(3H)one; furazlocillin; cis- 2-hexyl-5-methyl-3,4,5,6a,7,8,9,9a- octahydrocyclopent[4,5]-imidazo[2,1-b]purin-4-
- PDE5 inhibitors for use with the invention are selected from the group:
- a particularly preferred PDE5 inhibitor is 5-[2-ethoxy-5-(4-methyl-1 - piperazinylsulphonyl)phenyl]-1-methyl-3-n-propyl-1 ,6-dihydro-7H-pyrazolo[4,3- d]pyrimidin-7-one (sildenafil) (also known as 1-[[3-(6,7-dihydro-1-methyl-7-oxo-3- propyl-1H-pyrazolo[4,3-d]pyrimidin-5-yl)-4-ethoxyphenyl]sulphonyl]-4- methylpiperazine) and pharmaceutically acceptable salts thereof.
- Sildenafil citrate is a preferred salt.
- the term "the 5HT1 a agonist” means the 5HT1a agonists for use with the invention.
- the term includes pharmaceutically acceptable salts, solvates and polymorphs of the 5HT1a agonists for use with the invention.
- the suitability of the 5HT1a agonists can be readily determined by evaluation of its potency and selectivity using literature methods followed by evaluation of its toxicity, absorption, metabolism, pharmacokinetics, etc in accordance with standard pharmaceutical practice.
- the 5HT1a agonists have an affinity for the recombinant human 5HT1a receptor with a Ki of less than or equal to 300nM, preferably with a Ki of less than or equal tolOOnM, more preferably with a Ki of less than or equal to 30nM, yet more, preferably with a Ki of less than or equal to 10nM, most preferably with a Ki of less than or equal to 1nM.
- EC50 values for the 5HT1a agonists may be determined using the 5HT1a assay in the Test Methods Section hereinafter.
- the agonists have an EC50 less than or equal to 300nM, preferably with an EC50 of less than or equal tolOOnM, more preferably with an EC50 of less than or equal to 30nM, yet more preferably with an EC50 of less than or equal to 10nM, most preferably with a EC50 of less than or equal to 1nM.
- the 5HT1a agonists are selective for the 5HT1a receptor over alphaadrenoceptors and dopamine.
- Examples of 5HT1 a agonists for use with the invention are:
- Zaprasidone buspirone HCI, Urapidil, Tandosporine, Sunepitron, Ebalzotan, Ipsapirone, Zalospirone, Gepirone, Repinotan, Alnespirone, MKC242, Eptapirone, SR57746A, AP-521 , SUN-N4057, Lesopitron, DU-125530, VML-670, Flesinoxan, E6265, Flibanserin, buspar, AP-521 , SUN-N4057, LY293284, LY301317 and 8-OH- DPAT.
- Flibanserin Particularly preferred is Sildenafil or 2-(Methoxyethyl)-5-[2-ethoxy-5- (4-ethylpiperazin-1-ylsulfonyl)pyridin-3-yl]-3-ethyl-2,6-dihydro-7H-pyrazolo[4,3- d]pyrimidin-7-one with Flibanserin.
- Oral bioavailablity refers to the proportion of an orally administered drug that reaches the systemic circulation.
- the factors that determine oral bioavailabiiity of a drug are dissolution, membrane permeability and metabolic stability.
- a screening cascade of firstly in vitro and then in vivo techniques is used to determine oral bioavailablity.
- the solubilisation of the drug by the aqueous contents of the gastrointestinal tract can be predicted from in vitro solubility experiments conducted at appropriate pH to mimic the GIT.
- the PDE5 inhibitors Preferably have a minimum solubility of 50 mcg/ml. Solubility can be determined by standard procedures known in the art such as described in Adv. Drug Deliv. Rev. 23, 3-25, 1997.
- Membrane permeability refers to the passage of a compound through the cells of the GIT. Lipophilicity is a key property in predicting this and is defined by in vitro Log D .4 measurements using organic solvents and buffer.
- the PDE5 inhibitors Preferably have a Log D 7 . 4 of -2 to +4, more preferably -1 to +3.
- the log D can be determined by standard procedures known in the art such as described in J. Pharm. Pharmacol. 1990, 42:144.
- Cell monolayer assays such as CaCo 2 add substantially to prediction of favourable membrane permeability in the presence of efflux transporters such as p- glycoprotein, so-called caco-2 flux.
- the PDE5 inhibitors have a caco-2 flux of greater than 2x10 "6 cms "1 , more preferably greater than 5x10 ⁇ 6 cms "1 .
- the caco flux value can be determined by standard procedures known in the art such as described in J. Pharm. Sci, 1990, 79, 595-600 Metabolic stability addresses the ability of the GIT or the liver to metabolise compounds during the absorption process: the first pass effect.
- Assay systems such as microsomes, hepatocytes etc are predictive of metabolic liability.
- the PDE5 inhibitors show metabolic stability in the assay system that is commensurate with an hepatic extraction of less then 0.5. Examples of assay systems and data manipulation are described in Curr. Opin. Drug Disc. Devel., 201 , 4, 36-44, Drug Met. Disp.,2000, 28, 1518-1523
- Absolute bioavailabiiity is determined in these studies by administering the compound separately or in mixtures by the oral route. For absolute determinations (% absorbed) the intravenous route is also employed. Examples of the assessment of oral bioavailabiiity in animals can be found in Drug Met. Disp.,2001 , 29, 82-87; J. Med Chem , 1997, 40, 827-829, Drug Met. Disp.,1999, 27, 221-226.
- the PDE5 inhibitors and 5HT1 a agonists may also be combined with one or more additional active agents for treating sexual dysfunction, particularly FSAD in subjects with concurrent significant HSDD.
- the additional active agents may be selected from the following list: 1) one or more naturally occurring or synthetic prostaglandins or esters thereof (suitable prostaglandins for use herein include compounds such as alprostadil, prostaglandin E ⁇ , prostaglandin Eo, 13, 14 - dihydroprosta glandin E-i, prostaglandin E 2 , eprostinol, natural synthetic and semi-synthetic prostaglandins and derivatives thereof including those described in WO- 00033825 and/or US 6,037,346 issued on 14th March 2000 all incorporated herein by reference, PGE 0 , PGEi, PGA ⁇ PGB-i, PGFi ⁇ , 19-hydroxy PGAi, 19-hydroxy - PGBi, PGE 2 , PGB 2 , 19-hydroxy-PGA 2 ,
- NO-donor compounds include organic nitrates, such as mono- di or tri- nitrates or organic nitrate esters including glyceryl brinitrate (also known as nitroglycerin), isosorbide 5-mononitrate, isosorbide dinitrate, pentaerythritol tetranitrate, erythrityl tetranitrate, sodium nitroprusside (SNP), 3- morpholinosydnonimine molsidomine, S-nitroso- N-acetyl penicilliamine (SNAP) S-nitroso-N-glutathione (SNO-GLU), N-hydroxy - L-arginine, amylnitrate, linsidomine, linsidomine chlorohydrate, (SIN-1) S-nitroso - N- cysteine, diazenium diolates
- organic nitrates such as mono- di or tri- nitrates
- potassium channel openers or modulators include nicorandil, cromokalim, levcromakalim, lemakalim, pinacidil, cliazoxide, minoxidil, charybdotoxin, glyburide, 4-aminopyridine, BaCI 2 ) ; 5) one or more dopaminergic agents, preferably apomorphine or a selective D 2 , D 3 or D 2 /D 3 agonist such as, pramipexole and ropirinol (as claimed in WO- 0023056), PNU95666 (as claimed in WO-0040226);
- vasodilator agents suitable vasodilator agents for use herein include nimodepine, pinacidil, cyclandelate, isoxsuprine, chloroprumazine, halo peridol, Rec 15/2739, trazodone);
- ergot alkoloids suitable ergot alkaloids are described in US patent 6,037,346 issued on 14th March 2000 and include acetergamine, brazergoline, bromerguride, cianergoline, delorgotrile, disulergine, ergonovine maleate, ergotamine tartrate, etisulergine, lergotrile, lysergide, mesulergine, metergoline, metergotamine, nicergoline, pergolide, propisergide, proterguride, terguride);
- Atrial naturetic factor also known as atrial naturetic peptide
- B type and C type naturetic factors such as inhibitors or neutral endopeptidase (see later);
- angiotensin receptor antagonists such as losartan
- one or more substrates for NO-synthase such as L-arginine
- one or more cholesterol lowering agents such as statins (e.g. atorvastatin/Lipitor- trade mark) and fibrates;
- one or more antiplatelet and antithrombotic agents e.g. tPA, uPA, warfarin, hirudin and other thrombin inhibitors, heparin, thromboplastin activating factor inhibitors; 16) one or more insulin sensitising agents such as rezulin and hypoglycaemic agents such as glipizide; 17) one or more acetylcholinesterase inhibitors such as donezipil;.
- one or more estrogen receptor modulators and/or estrogen agonists and/or estrogen antagonists preferably raloxifene, tibolone or lasofoxifene, (-)-cis-6- phenyl-5-[4-(2-pyrrolidin-1-yl-ethoxy)-phenyl]-5,6,7,8-tetrahydronaphthalene- 2-ol and pharmaceutically acceptable salts thereof the preparation of which is detailed in WO 96/21656; 19) one or more further PDE inhibitors, particularly a PDE 2, 7 or 8 inhibitor, preferably a PDE2 inhibitor, said inhibitors preferably having an IC50 against the respective enzyme of less than 100nM;
- NPY neuropeptide Y
- NPY1 or NPY5 inhibitor preferably NPY1 inhibitor
- said NPY inhibitors having an IC50 of less than 100nM , more preferably less than 50nM (an assay for identifying NPY inhibitors is presented in WO-A-98/52890 (see page 96, lines 2 to 28);
- VIP vasoactive intestinal protein
- VIP mimetic vasoactive intestinal protein
- VIP analogue more particularly mediated by one or more of the VIP receptor subtypes VPAC1 NPAC or PACAP (pituitory adenylate cyclase activating peptide), one or more of a VIP receptor agonist or a VIP analogue (eg Ro-125-1553) or a VIP fragment, one or more of a ⁇ -adrenoceptor antagonist with VIP combination eg Invicorp, Aviptadil);
- a melanocortin receptor agonist or modulator or melanocortin enhancer such as melanotan II, PT-14, PT-141 or compounds claimed in WO-09964002, WO-00074679, WO-09955679, WO-00105401 , WO- 00058361 , WO-00114879, WO-00113112, WO-09954358;
- a serotonin receptor agonist, antagonist or modulator more particularly agonists, antagonists or modulators for example 5HT2A, 5HT2C, 5HT3, 5HT6 and/or 5HT7 receptors, including those described in WO- 09902159, WO-00002550 and/or WO-00028993;
- an androgen such as androsterone, dehydro-androsterone, testosterone, androstanedione and a synthetic androgen;
- an androgen receptor modulator for example tibolone
- 26 one or more of an oestrogen, such as oestradiol, oestrone, oestriol and a synthetic estrogen, such as oestrogen benzoate);
- a modulator of transporters for noradrenaline, dopamine and/or serotonin such as bupropion, GW-320659;
- a purinergic receptor agonist and/or modulator 29 one or more of a neurokinin (NK) receptor antagonist, including those described in WO-09964008;
- an opioid receptor agonist, antagonist or modulator preferably agonists for the ORL-1 receptor
- an agonist or modulator for oxytocin/vasopressin receptors preferably a selective oxytocin agonist or modulator
- NEP inhibitors preferably wherein said NEP is EC 3.4.24J 1 and more preferably wherein said NEP inhibitor is a selective inhibitor for EC 3.4.24 J 1 , more preferably a selective NEP inhibitor is a selective inhibitor for EC 3.4.24.11 , which has an IC 50 of less than 100nM (e.g.
- NEP inhibitor compounds are described in EP-A- 1097719; IC50 values against NEP and ACE may be determined using methods described in published patent application EP1097719-A1 , paragraphs [0368] to [0376]; 34) one or more compounds which inhibit angiotensin-converting enzyme such as enalapril, and one or more combined inhibitors of angiotensin-converting enzyme and neutral endopeptidase such as omapatrilat;
- ACE angiotensin-converting enzyme
- the PDE5 inhibitors (particularly sildenafil) and the 5HT1a agonist may be combined with one or more active agents selected from the following list: i) one or more of an androgen such as androsterone, dehydro-androsterone, testosterone, androstanedione and a synthetic androgen; ii) one or more of an oestrogen, such as oestradiol, oestrone, oestriol and a synthetic estrogen, such as oestrogen benzoate); iii) one or more NEP inhibitors, preferably wherein said NEP is EC 3.4.24J 1 and more preferably wherein said NEP inhibitor is a selective inhibitor for EC 3.4.24J 1 , more preferably a selective NEP inhibitor is a selective inhibitor for EC 3.4.24.11 , which has an IC 50 of less than 100nM (e.g.
- suitable NEP inhibitor compounds are described in EP-A- 1097719; v) one or more of an NPY1 having an IC50 of less than 100nM , more preferably less than 50nM, for examples see published European Patent Application EP1 097 718 A1 ; vi) one or more estrogen receptor modulators and/or estrogen agonists and/or estrogen antagonists, preferably raloxifene, tibolone or lasofoxifene, (-)-cis-6- phenyl-5-[4-(2-pyrrolidin-1-yl-ethoxy)-phenyl]-5,6,7,8-tetrahydronaphthalene- 2-ol and pharmaceutically acceptable salts thereof the preparation of which is detailed in WO 96/21656; vii) one or more of a melanocortin receptor agonist or modulator or melanocortin enhancer, such as melanotan II, PT-14, PT
- Particularly preferred combinations for treating FSAD in subjects with concurrent significant HSDD are: Sildenalfil, Flibanserin and an androgen; sildenafil, Flibanserin and an oestrogen; sildenafil, , Flibanserin an androgen and an oestrogen; Idenafi , Flibanseri n and lasofoxifene; ildenafi , Flibanseri n, lasofox ifene and an androgen; ildenafi , Flibanseri n, lasofox ifene and an oestrogen; or ildenafi , Flibanseri n, lasofox ifene, an androgen and an oestrogen; Idenafi , Flibanserin and a NEP nhibitor; Idenafi I, Flibanseri n, a NEP inh bitor and an androgen; Idenaf
- PDE5 inhibitors with 5HT1a agonists and combinations thereof can be administered alone but will generally be administered in admixture with a suitable pharmaceutical excipient, diluent or carrier selected with regard to the intended route of administration and standard pharmaceutical practice.
- the PDE5 inhibitors with 5HT1a agonists and combinations thereof can be administered orally, buccally or sublingually in the form of tablets, capsules, multi-particulates, gels, films, ovules, elixirs, solutions or suspensions, which may contain flavouring or colouring agents, for immediate-, delayed-, modified-, sustained-, pulsed- or controlled-release applications.
- the PDE5 inhibitors with 5HT1a agonists and combinations thereof may also be administered as fast- dispersing or fast-dissolving dosage forms or in the form of a high energy dispersion or as coated particles. Suitable formulations may be in coated or uncoated form, as desired.
- Such solid pharmaceutical compositions may contain excipients such as microcrystalline cellulose, lactose, sodium citrate, calcium carbonate, dibasic calcium phosphate, glycine and starch (preferably corn, potato or tapioca starch), disintegrants such as sodium starch glycollate, croscarmellose sodium and certain complex silicates, and granulation binders such as polyvinylpyrrolidone, hydroxypropylmethylcellulose (HPMC), hydroxypropylcellulose (HPC), sucrose, gelatin and acacia. Additionally, lubricating agents such as magnesium stearate, stearic acid, glyceryl behenate and talc may be included.
- excipients such as microcrystalline cellulose, lactose, sodium citrate, calcium carbonate, dibasic calcium phosphate, glycine and starch (preferably corn, potato or tapioca starch), disintegrants such as sodium starch glycollate, croscarmellose sodium and certain complex silicates, and
- Active ingredient means a PDE5 inhibitor with 5HT1a agonists or combination thereof.
- a tablet is prepared using the following ingredients :
- Active ingredient 50 mg is blended with cellulose (microcrystalline), silicon dioxide, stearic acid (fumed) and the mixture is compressed to form tablets.
- An intravenous formulation may be prepared by combining active ingredient (100 mg) with isotonic saline (1000 ml)
- the tablets are manufactured by a standard process, for example, direct compression or a wet or dry granulation process.
- the tablet cores may be coated with appropriate overcoats.
- Solid compositions of a similar type may also be employed as fillers in gelatin or HPMC capsules.
- Preferred excipients in this regard include lactose, starch, a cellulose, milk sugar or high molecular weight polyethylene glycols.
- the PDE5 inhibitors with 5HT1a agonists may be combined with various sweetening or flavouring agents, colouring matter or dyes, with emulsifying and/or suspending agents and with diluents such as water, ethanol, propylene glycol and glycerin, and combinations thereof.
- Modified release and pulsatile release dosage forms may contain excipients such as those detailed for immediate release dosage forms together with additional excipients that act as release rate modifiers, these being coated on and/or included in the body of the device.
- Release rate modifiers include, but are not exclusively limited to, hydroxypropylmethyl cellulose, methyl cellulose, sodium carboxymethylcellulose, ethyl cellulose, cellulose acetate, polyethylene oxide, Xanthan gum, Carbomer, ammonio methacrylate copolymer, hydrogenated castor oil, camauba wax, paraffin wax, cellulose acetate phthalate, hydroxypropylmethyl cellulose phthalate, methacrylic acid copolymer and mixtures thereof.
- Modified release and pulsatile release dosage forms may contain one or a combination of release rate modifying excipients.
- Release rate modifying excipients may be present both within the dosage form i.e. within the matrix, and/or on the dosage form, i.e. upon the surface or coating.
- Fast dispersing or dissolving dosage formulations may contain the following ingredients: aspartame, acesulfame potassium, citric acid, croscarmellose sodium, crospovidone, diascorbic acid, ethyl acrylate, ethyl cellulose, gelatin, hydroxypropylmethyl cellulose, magnesium stearate, mannitol, methyl methacrylate, mint flavouring, polyethylene glycol, fumed silica, silicon dioxide, sodium starch glycolate, sodium stearyl fumarate, sorbitol, xylitol.
- dispersing or dissolving as used herein to describe FDDFs are dependent upon the solubility of the drug substance used i.e. where the drug substance is insoluble a fast dispersing dosage form can be prepared and where the drug substance is soluble a fast dissolving dosage form can be prepared.
- the PDE5 inhibitors with 5HT1a agonists and combinations thereof can also be administered parenterally, for example, intracavemouslly, intravenously, intra- arterially, intraperitoneally, intrathecally, intraventricularly, intraurethrally, intrasternally, intracranially, intramuscularly or subcutaneously, or they may be administered by infusion or needleless injection techniques.
- parenteral administration they are best used in the form of a sterile aqueous solution which may contain other substances, for example, enough salts or glucose to make the solution isotonic with blood.
- the aqueous solutions should be suitably buffered (preferably to a pH of from 3 to 9), if necessary.
- the preparation of suitable parenteral formulations under sterile conditions is readily accomplished by standard pharmaceutical techniques well-known to those skilled in the art.
- dosage levels and other dosage levels herein are for the average human subject having a weight range of about 65 to 70 kg.
- the skilled person will readily be able to determine the dosage levels required for a subject whose weight falls outside this range, such as children and the elderly.
- the dosage of the PDE5 inhibitor with 5HT1a agonists in such formulations will depend on its potency, but can be expected to be in the range of from 1 to 500 mg for administration up to three times a day.
- a preferred dose is in the range 10 to 100 mg (e.g. 10, 25, 50 and 100 mg) which can be administered once, twice or three times a day (preferably once).
- the precise dose will be as determined by the prescribing physician and will depend on the age and weight of the subject and severity of the symptoms.
- the daily dosage level of the PDE5 inhibitors will usually be from to 5 to 500 mg/kg (in single or divided doses).
- tablets or capsules may contain from 5 mg to 250 mg (for example 10 to 100 mg) of the PDE5 inhibitor for administration singly or two or more at a time, as appropriate.
- the physician in any event will determine the actual dosage which will be most suitable for any individual patient and it will vary with the age, weight and response of the particular patient.
- the above dosages are exemplary of the average case. There can, of course, be individual instances where higher or lower dosage ranges are merited and such are within the scope of this invention.
- the PDE5 inhibitors may be taken as a single dose as needed or desired (i.e. prn). It is to be appreciated that all references herein to treatment include acute treatment (taken as required) and chronic treatment (longer term continuous treatment).
- PDE5 inhibitors with 5HT1a agonists and combinations thereof can also be administered intranasally or by inhalation and are conveniently delivered in the form of a dry powder inhaler or an aerosol spray presentation from a pressurised container, pump, spray, atomiser or nebuliser, with or without the use of a suitable propellant, e.g.
- the dosage unit may be determined by providing a valve to deliver a metered amount.
- the pressurised container, pump, spray, atomiser or nebuliser may contain a solution or suspension of the active compound, e.g.
- Capsules and cartridges (made, for example, from gelatin) for use in an inhaler or insufflator may be formulated to contain a powder mix of the PDE5 inhibitor and a suitable powder base such as lactose or starch.
- Aerosol or dry powder formulations are preferably arranged so that each metered dose or "puff contains from 1 ⁇ g to 50 mg of a PDE5 inhibitor for delivery to the patient.
- the overall daily dose with an aerosol will be in the range of from 1 ⁇ g to 50 mg which may be administered in a single dose or, more usually, in divided doses throughout the day.
- the PDE5 inhibitors with 5HT1a agonists and combinations thereof can be administered in the form of a suppository or pessary, or they may be applied topically in the form of a gel, hydrogel, lotion, solution, cream, ointment or dusting powder.
- the PDE5 inhibitors with 5HT1a agonists and combinations thereof may also be dermally or transdermally administered, for example, by the use of a skin patch, depot or subcutaneous injection. They may also be administered by the pulmonary or rectal routes.
- the PDE5 inhibitors with 5HT1a agonists and combinations thereof can be formulated as a suitable ointment containing the active compound suspended or dissolved in, for example, a mixture with one or more of the following: mineral oil, liquid petrolatum, white petrolatum, propylene glycol, polyoxyethylene polyoxypropylene compound, emulsifying wax and water.
- ком ⁇ онентs can be formulated as a suitable lotion or cream, suspended or dissolved in, for example, a mixture of one or more of the following: mineral oil, sorbitan monostearate, a polyethylene glycol, liquid paraffin, polysorbate 60, cetyl esters wax, cetearyl alcohol, 2-octyldodecanol, benzyl alcohol and water.
- the PDE5 inhibitors with 5HT1a agonists and combinations thereof may also be used in combination with a cyclodextrin.
- Cyclodextrins are known to form inclusion and non-inclusion complexes with drug molecules. Formation of a drug-cyclodextrin complex may modify the solubility, dissolution rate, bioavailabiiity and/or stability property of a drug molecule. Drug-cyclodextrin complexes are generally useful for most dosage forms and administration routes.
- the cyclodextrin may be used as an auxiliary additive, e.g. as a carrier, diluent or solubiliser.
- Alpha-, beta- and gamma-cyclodextrins are most commonly used and suitable examples are described in WO-A-91/11172, WO- A-94/02518 and WO-A-98/55148.
- Oral administration of the PDE5 inhibitors with 5HT1a agonists and combinations thereof is a preferred route, being the most convenient.
- the drug may be administered parenterally, sublingually or buccally.
- Transdermal administration of the PDE5 inhibitors with 5HT1a agonists and combinations thereof is a further preferred route, particularly local to the female genitalia, preferably intravaginally.
- a preferred method of transdermal administration of oestrogen and testosterone is using a skin patch, depot or implants.
- a preferred dose of an estrogen for combination with the PDE5 inhibitor and 5HT1a agonist is in the range 0 to 5 mg per day.
- a preferred dose of an androgen for combination with the PDE5 inhibitor and 5HT1 a agonist is in the range 0 to 25 mg per day.
- the invention since the invention has an embodiment that relates to treatment of sexual dysfunction, with a combination of compounds which may be co-administered separately, the invention also relates to combining separate pharmaceutical compositions in kit form. Therefore according to a further aspect, the invention provides a kit comprising: a) a first pharmaceutical composition comprising a PDE5 inhibitor and a pharmaceutically acceptable carrier or diluent; b) a second pharmaceutical composition comprising 5HT1a agonist and a pharmaceutically acceptable carrier or diluent; and a container for the two compositions.
- the inventi on since the inventi on has an embodiment that relates to treatment of FSAD with concomitant HSDD, wi ith a combination of compounds which may be co-administered separately, the inventi on also relates to combining separate pharmaceutical compositions in kit form.
- the invention provides a kit comprising: a) a first pharmaceutical composition comprising a PDE5 inhibitor and a pharmaceutically acceptable carrier or diluent; b) a second pharmaceutical composition comprising 5HT1a agonist and a pharmaceutically acceptable carrier or diluent; c) a third pharmaceutical composition comprising an androgen and a pharmaceutically acceptable carrier or diluent; d) a fourth pharmaceutical composition comprising an oestrogen and a pharmaceutically acceptable carrier or diluent and a container for the four compositions.
- the four compositions are separate components intended for co-administration to a female subject suffering from FSAD, wherein the patient has concentrations of hormone less than the physiological levels found in a normal pre-menopausal woman.
- co- administration it is meant that the four components can be taken from the kit and combined for administration together as a composition or as part of the same, unitary dosage form, such as an parenterally or orally administered solution.
- Co- administration also includes administering the components separately (e.g. as tablets or capsules), but as part of the same therapeutic treatment program or regimen.
- Separatate administration is the preferred mode of administration. The four components need not be administered at essentially the same time, although they can be if so desired.
- co-administration includes, for example administering all four components as separate dosages or dosage forms and at essentially the same time.
- Co-administration also includes separate administration at different times, in any order, and if preferred by different routes of administration.
- the four components be administered at essentially the same time. If administered separately and at different times, it is preferred that the four components be administered within 24 hours of each other. If administered separately, It is preferred that the four components be administered by the same route.
- An example of a kit is the so-called blister pack well known in the packaging industry particularly for packaging pharmaceutical dosage forms.
- a PDE5 inhibitor with a 5HT1a agonist for treating sexual dysfunction ii) a PDE5 inhibitor with a 5HT1a agonist for treating FSAD in a subject who has concurrent significant HSDD; iii) a pharmaceutical combination (for simultaneous, separate or sequential administration) for treating sexual dysfunction comprising a PDE5 inhibitor and a 5HT1 a agonist, an oestrogen, an androgen and optionally an additional active agent as hereinabove defined; iv) a pharmaceutical combination (for simultaneous, separate or sequential administration) for treating FSAD in a subject who has concurrent significant HSDD comprising a PDE5 inhibitor, a 5HT1a agonist, an oestrogen, an androgen and optionally an additional active agent as hereinabove defined;
- a pharmaceutical combination for the manufacture of a medicament for treating FSAD in a subject who has concurrent significant HSDD comprising a PDE5 inhibitor, a 5HT1a agonist, an oestrogen, an androgen and optionally an additional active agent as hereinabove defined;
- kits for treating FSAD in a subject who does not have concurrent significant HSDD comprising: a) a first pharmaceutical composition comprising a PDE5 inhibitor; b) a second pharmaceutical composition comprising a 5HT1a agonist; c) a third pharmaceutical composition comprising an androgen; d) a fourth pharmaceutical composition comprising an oestrogen; e) optionally a pharmaceutical composition comprising an additional active agent as hereinabove defined; and f) a container for the compositions;
- a method of treating FSAD in a subject who has concurrent significant HSDD comprising treating said patient with an effective amount of a PDE5 inhibitor and a 5HT1a agonist;
- a method of treating FSAD in a subject who has concurrent significant HSDD comprising treating said patient with pharmaceutical combination comprising a PDE5 inhibitor, a 5HT1a agonist, an oestrogen, an androgen and optionally an additional active agent as hereinabove defined; and'
- a method of treating FSAD in a subject who has concurrent significant HSDD comprising the steps of: a) measuring the subject's physiological levels of oestrogen and androgen; b) if not replete, administering to the subject an oestrogen and/or an androgen until replete levels are achieved; then c) administering a PDE5 inhibitor and a 5HT1a agonist.
- PDE action potency values referred to herein are determined by the following assays.
- Preferred PDE compounds suitable for use in accordance with the present invention are potent and selective PDE5 inhibitors.
- In vitro PDE inhibitory activities against cyclic guanosine 3',5'-monophosphate (cGMP) and cyclic adenosine 3', 5'- monophosphate (cAMP) phosphodiesterases can be determined by measurement of their IC 5 o values (the concentration of compound required for 50% inhibition of enzyme activity).
- the required PDE enzymes can be isolated from a variety of sources, including human corpus cavernosum, human and rabbit platelets, human cardiac ventricle, human skeletal muscle and bovine retina, essentially by the method of W.J. Thompson and M.M. Appleman (Biochem., 1971 , 10, 311).
- the cGMP-specific PDE (PDE5) and the cGMP-inhibited cAMP PDE (PDE3) can be obtained from human corpus cavernosum tissue, human platelets or rabbit platelets; the cGMP-stimulated PDE (PDE2) was obtained from human corpus cavernosum; the calcium/calmodulin (CaACAM)-dependent PDE (PDE1) from human cardiac ventricle; the cAMP-specific PDE (PDE4) from human skeletal muscle; and the photoreceptor PDE (PDE6) from bovine retina.
- Phosphodiesterases 7-11 can be generated from full length human recombinant clones transfected into SF9 cells.
- Assays can be performed either using a modification of the "batch” method of W.J. Thompson et al. (Biochem., 1979, 18, 5228) or using a scintillation proximity assay for the direct detection of AMP/GMP using a modification of the protocol described by Amersham pic under product code TRKQ7090/7100.
- the final assay volume was made up to 100 ⁇ l with assay buffer [20 mM Tris-HCI pH 7.4, 5 mM MgCI 2 , 1 mg/ml bovine serum albumin]. Reactions were initiated with enzyme, incubated for 30-60 min at 30°C to give ⁇ 30% substrate turnover and terminated with 50 ⁇ l yttrium silicate SPA beads (containing 3 mM of the respective unlabelled cyclic nucleotide for PDEs 9 and 11).
- Suitable assays to identify 5HT1a agonists are disclosed in J Pharmacol Exp Ther. 1998, 284(3), 1082-1094 and in J Pharmacol Toxicol Methods 1998, 40(1), 47-55. Other suitable assays are well known to the man skilled in the art.
- Diagnosis of FSAD with concomitant HSDD may be achieved through the use of the Sexual History Interview , administered by sexual health experts for the FSD diagnosis of potential subjects.
- the SHI was developed by a team of internal clinical personnel at Pfizer and external sexual health experts. The SHI addresses two main aspects relevant to subject inclusion/exclusion; identification of the sub- component of FSD and psychosexual eligibility. These two aspects are key to ensuring appropriate identification of the target population and that the main inclusion and exclusion criteria relevant to psychosexual eligibility are met.
- the SHI is detailed hereinafter as Appendix 2.
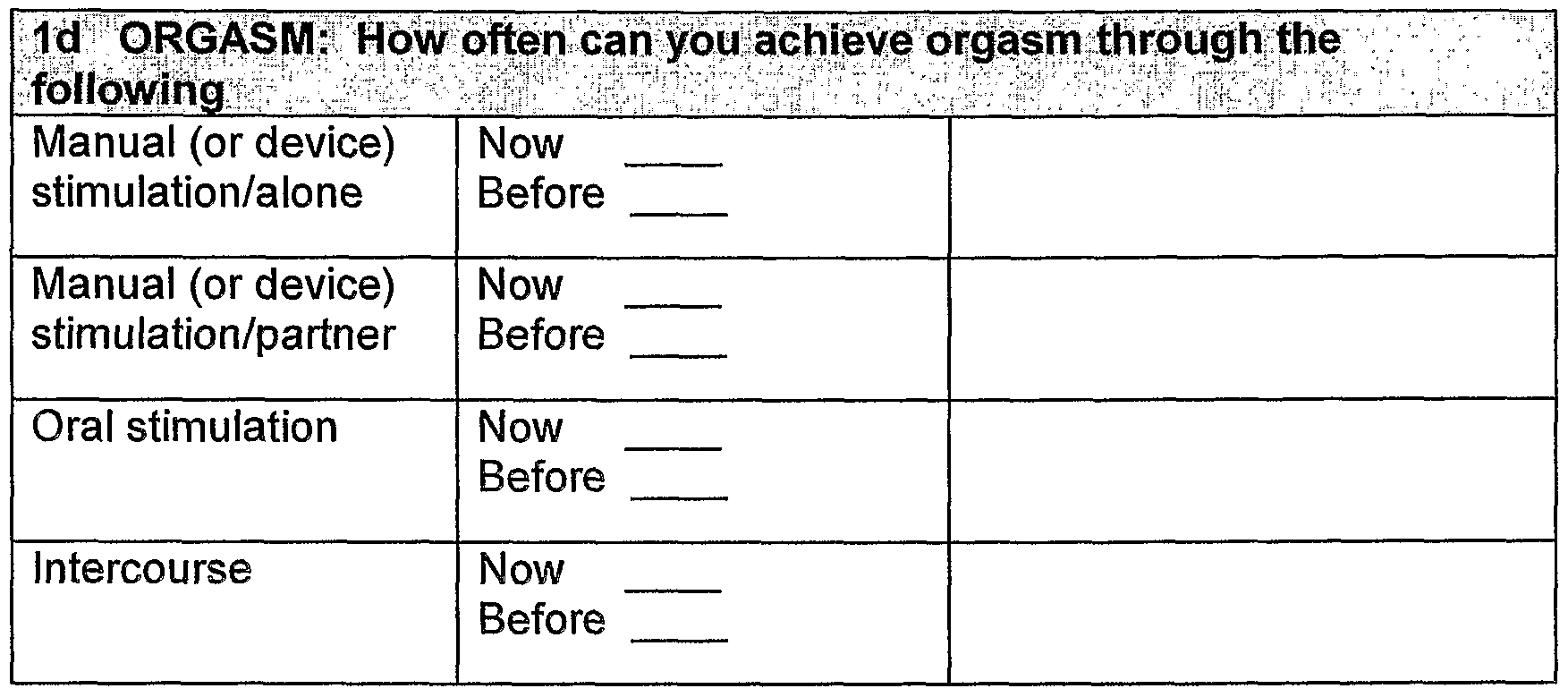
- the Female Sexual Function Questionnaire (SFQ)
- the Female Sexual Function Questionnaire is a self-report outcomes measure of female sexual function that has been developed to be multi-dimensional and subject-centered.
- the SFQ addresses all aspects of the sexual response cycle (desire, arousal, orgasm) as well as pain, which is in keeping with the DSM-IV diagnostic criteria and the newly generated AFUD definitions 1 .
- the item content of the SFQ was generated from the aggregated responses of 82 women to a semi-structured interview.
- the content of the interview addressed, amongst other things, women's understanding of the terms commonly used to describe the phases of sexual response (e.g. desire and arousal) and the language that they themselves used to describe these changes.
- These interviews also addressed some of the consequences of female sexual dysfunction (FSD) for the woman, her partner and their relationship and some of these core issues are also represented within the SFQ item content.
- the validity of the SFQ at both the item level and the domain level supports the use of individual SFQ domains as primary endpoints (e.g. Arousal or Orgasm) with the remaining domains or individual items being utilised as secondary endpoints. This approach also ensures that all aspects of sexual function are evaluated in a therapeutic area in which the effects of dysfunction and intervention are not currently wholly understood.
- primary endpoints e.g. Arousal or Orgasm
- the SFQ has been developed and validated in a number of languages (18) as well as for use in the USA and Australia.
- the SFQ contains 34 items and each item has between 5 or 7 possible response options.
- Items 1-5, 27-28, and 33-34 are scored 1-5 (in ascending order) e.g. 1. Over the last 4 weeks, how often have you had pleasurable thoughts and feelings about sexual activity?
- Items 6-14, 16, 20-21 , 23-26 are scored 1-5 (in ascending order) with the 'not applicable' category (e.g. 'I did not take part in sexual activity', I did not have any orgasms') set to 'missing'. e.g.
- Items 15 and 19 are scored 0-6 (in ascending order) e.g.
- Item 22 is scored from 5-1 with the 'I did not take part in sexual activity' scored as 'missing' and the 'I did not take part in sexual activity because of being concerned or anxious about pain' scored as 0 i.e. 22. Over the last 4 weeks, how often have you been concerned or anxious about pain during sexual activity? I did not take part in sexual activity (missing) I did not take part in sexual activity because of being concerned or anxious about pain' (0) Not at all Sometimes Often Very often Every time Note: Item 32 is not included in the overall scoring but may be tabulated if desired.
- Total Score A total score may be derived from summing the individual item score for each item, except item 32. The total score range is 30-167. A higher score indicates better sexual function.
- the SFQ scores When used in conjunction with a clinical sexual history interview the SFQ scores should be supportive of information derived from the subject (i.e. if the subject proposes that orgasm is her greatest sexual complaint a score within the range of 3- 11 would be expected. A score greater than 12 should prompt a review and further discussion). Where discrepancies between the SFQ score and the sexual problem (s) derived from the sexual history interview arise the opportunity should be taken to discuss this further with the subject and determine the cause(s) for any discrepancy.
- Sexual Activity includes any activity which may result in sexual stimulation or sexual pleasure e.g. intercourse, caressing, foreplay, masturbation (i.e. self masturbation or your partner masturbating you) and oral sex (i.e. your partner giving you oral sex).
- masturbation i.e. self masturbation or your partner masturbating you
- oral sex i.e. your partner giving you oral sex
- Sexual Activity Includes any activity which may result in sexual stimulation or sexual pleasure, e.g. intercourse, caressing, foreplay, masturbation (i.e. self- masturbation or your partner masturbating you) and oral sex (i.e. your partner giving you oral sex).
- Question 1 can EITHER be treated as open-ended, with you checking all options volunteered & prompting for items not mentioned OR subject can fill in directly, then you review answers together.
- a fully annotated synopsis of appropriate length is requested for the following three questions. You are not limited to the space provided. All text must reference consistently to the subject's answers to specific questions & to interviewer annotations, as appropriate. The text must be legible to/auditable by, a Pfizer or country regulatory agent. If a subject is recommended for study inclusion, the text must justify why any potentially exclusionary information was considered less relevant. Please keep in mind that if you think the subject's problem is primarily ascribable to an emotional or relationship issue, to the partner in any way (e.g. is situational), or is a question of sexual enthusiasm, she is unlikely to benefit from study drug treatment and by protocol must be excluded.
- DSM-IV definitions Hypoactive Sexual Desire Disorder Persistently or recurrently deficient (or absent) sexual fantasies and desire for sexual activity. (Judgement of deficiency or absence is made by the clinician, taking into account factors that affect sexual functioning, such as age and the context of the person's life.) The disturbance causes marked distress or interpersonal difficulty The sexual dysfunction is not better accounted for by another clinical condition (other than another sexual dysfunction) and is not due exclusively to the direct physiological effects of a substance (e.g. a drug of abuse, a medication) or a general medical condition
- Female Sexual Arousal Disorder Persistent or recurrent inability to attain, or to maintain until completion of the sexual activity, an adequate lubrication-swelling response of sexual excitement.
- the disturbance causes marked distress or interpersonal difficulty
- the sexual dysfunction is not better accounted for by another clinical condition (except another sexual dysfunction) and is not due exclusively to the direct physiological effects of a substance (e.g. a drug of abuse, a medication) or a general medical condition
- Female Orgasmic Disorder Persistent or recurrent delay in, or absence of, orgasm following a normal sexual excitement phase. (Women exhibit wide variability in the type or intensity of stimulation that triggers orgasm.)
- the diagnosis of Female Orgasmic Disorder should be based on the clinician's judgement that the woman's orgasmic capacity is less that would be reasonable for her age, sexual experience, and the adequacy of sexual stimulation she receives.
- the disturbance causes marked distress or interpersonal difficulty
- the orgasmic dysfunction is not better accounted for by another clinical condition (except another Sexual Dysfunction) and is not due exclusively to the direct physiological effects of a substance (e.g. a drug of abuse, a medication) or a general medical condition
- Dyspareunia Recurrent or persistent genital pain associated with sexual intercourse The disturbance causes marked distress or interpersonal difficulty
- the dysfunction is not better accounted for by vaginismus or another clinical condition (except another Sexual Dysfunction) and is not due exclusively to the direct physiological effects of a substance (e.g. a drug of abuse, a medication) or a general medical condition.
Abstract
Description












Claims
Priority Applications (5)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| JP2006520035A JP2007516949A (en) | 2003-07-16 | 2004-07-12 | Treatment of sexual dysfunction |
| BRPI0411985-1A BRPI0411985A (en) | 2003-07-16 | 2004-07-12 | treatment of sexual dysfunction |
| CA002532252A CA2532252A1 (en) | 2003-07-16 | 2004-07-12 | Treatment of sexual dysfunction |
| EP04743948A EP1653966A1 (en) | 2003-07-16 | 2004-07-12 | Treatment of sexual dysfunction |
| MXPA06000623A MXPA06000623A (en) | 2003-07-16 | 2004-07-12 | Treatment of sexual dysfunction. |
Applications Claiming Priority (6)
| Application Number | Priority Date | Filing Date | Title |
|---|---|---|---|
| GB0316673A GB0316673D0 (en) | 2003-07-16 | 2003-07-16 | Treatment of female sexual dysfunction |
| GB0316673.3 | 2003-07-16 | ||
| GB0318095.7 | 2003-08-01 | ||
| GB0318095A GB0318095D0 (en) | 2003-08-01 | 2003-08-01 | Treatment of sexual dysfunction |
| GB0321308.9 | 2003-09-11 | ||
| GB0321308A GB0321308D0 (en) | 2003-09-11 | 2003-09-11 | Treatment of sexual dysfunction |
Publications (1)
| Publication Number | Publication Date |
|---|---|
| WO2005007166A1 true WO2005007166A1 (en) | 2005-01-27 |
Family
ID=34084177
Family Applications (1)
| Application Number | Title | Priority Date | Filing Date |
|---|---|---|---|
| PCT/IB2004/002286 WO2005007166A1 (en) | 2003-07-16 | 2004-07-12 | Treatment of sexual dysfunction |
Country Status (7)
| Country | Link |
|---|---|
| EP (1) | EP1653966A1 (en) |
| JP (1) | JP2007516949A (en) |
| BR (1) | BRPI0411985A (en) |
| CA (1) | CA2532252A1 (en) |
| MX (1) | MXPA06000623A (en) |
| TW (1) | TW200505410A (en) |
| WO (1) | WO2005007166A1 (en) |
Cited By (19)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2005053697A2 (en) * | 2003-12-01 | 2005-06-16 | Akzo Nobel N.V. | Treatment of sexual disorders |
| WO2005102342A1 (en) * | 2004-04-22 | 2005-11-03 | Boehringer Ingelheim International Gmbh | New pharmaceutical compositions for the treatment of sexual disorders ii |
| EP1740180A1 (en) * | 2004-04-22 | 2007-01-10 | Boehringer Ingelheim Pharmaceuticals, Inc. | Use of flibanserin in the treatment of premenstrual and other female sexual disorders |
| WO2007048801A2 (en) * | 2005-10-29 | 2007-05-03 | Boehringer Ingelheim International Gmbh | Sexual desire enhancing medicaments comprising benzimidazolone derivatives |
| WO2007048803A1 (en) * | 2005-10-29 | 2007-05-03 | Boehringer Ingelheim International Gmbh | Benzimidazolone derivatives for the treatment of premenstrual and other female sexual disorders |
| WO2007128802A2 (en) * | 2006-05-09 | 2007-11-15 | Boehringer Ingelheim International Gmbh | Use of flibanserin for the treatment of post-menopausal sexual desire disorders |
| WO2008054213A2 (en) * | 2006-11-03 | 2008-05-08 | Emotional Brain B.V. | Use of testosterone and a 5-ht1a agonist in the treatment of sexual dysfunction |
| US8227453B2 (en) | 2004-05-11 | 2012-07-24 | Emotional Brain B.V. | Pharmaceutical formulations and uses thereof in the treatment of female sexual dysfunction |
| US8227471B2 (en) | 2001-10-20 | 2012-07-24 | Sprout Pharmaceuticals, Inc. | Treating sexual desire disorders with flibanserin |
| US8227476B2 (en) | 2005-08-03 | 2012-07-24 | Sprout Pharmaceuticals, Inc. | Use of flibanserin in the treatment of obesity |
| US8512748B2 (en) | 2006-08-25 | 2013-08-20 | Boehringer Ingelheim International Gmbh | Controlled release system and method for manufacturing the same |
| US8545886B2 (en) | 2006-08-14 | 2013-10-01 | Boehringer Ingelheim International Gmbh | Extended release tablet formulations of flibanserin and method for manufacturing the same |
| JP2013241463A (en) * | 2005-11-11 | 2013-12-05 | Emotional Brain Bv | Pharmaceutical combination comprising testosterone in treatment of female sexual dysfunction |
| EP2695932A1 (en) | 2012-08-08 | 2014-02-12 | Ab Nanol Technologies Oy | Grease composition |
| US8658207B2 (en) | 2006-08-14 | 2014-02-25 | Boehringer Ingelheim International Gmbh | Extended release tablet formulations of flibanserin and method for manufacturing the same |
| EP2896624A1 (en) | 2007-03-28 | 2015-07-22 | Atir Holding S.A. | Heterotricyclic compounds as serotonergic and/or dopaminergic agents and uses thereof |
| US9763936B2 (en) | 2006-06-30 | 2017-09-19 | Sprout Pharmaceuticals, Inc. | Flibanserin for the treatment of urinary incontinence and related diseases |
| US10166230B2 (en) | 2007-09-12 | 2019-01-01 | Sprout Pharmaceuticals Inc. | Treatment of vasomotor symptoms |
| US10675280B2 (en) | 2001-10-20 | 2020-06-09 | Sprout Pharmaceuticals, Inc. | Treating sexual desire disorders with flibanserin |
Families Citing this family (1)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| WO2020032988A1 (en) * | 2018-08-07 | 2020-02-13 | Ilysm, LLC | Compositions and methods for treating sexual dysfunction and enhancing sexual response and pleasure |
Citations (6)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20020052370A1 (en) * | 2000-07-06 | 2002-05-02 | Barber Christopher Gordon | Cyclopentyl-substituted glutaramide derivatives as inhibitors of neutral endopeptidase |
| WO2002072586A1 (en) * | 2001-03-09 | 2002-09-19 | Pfizer Limited | Pyrazolo'4,3-d-pyrimidine for inhibiting cgmp pde |
| WO2002074288A2 (en) * | 2001-03-15 | 2002-09-26 | Vernalis Research Limited | Treatment and prevention of sexual dysfunction resulting from ssri-therapy by using a tetrahydrobenz cd indole-6-carboxamide |
| US20030055070A1 (en) * | 1999-07-01 | 2003-03-20 | Wilma Harrison | Phosphodiesterase type 5 (PDE5) inhibitors for the treatment of selective serotonin reuptake inhibitor (SSR) induced sexual dysfunction |
| WO2003035072A1 (en) * | 2001-10-20 | 2003-05-01 | Boehringer Ingelheim Pharma Gmbh & Co. Kg | Use of flibanserin in the treatment of sexual disorders |
| WO2004041259A1 (en) * | 2002-11-06 | 2004-05-21 | Pfizer Limited | Treatment of female sexual dysfunction |
-
2004
- 2004-07-12 MX MXPA06000623A patent/MXPA06000623A/en not_active Application Discontinuation
- 2004-07-12 BR BRPI0411985-1A patent/BRPI0411985A/en not_active IP Right Cessation
- 2004-07-12 CA CA002532252A patent/CA2532252A1/en not_active Abandoned
- 2004-07-12 JP JP2006520035A patent/JP2007516949A/en active Pending
- 2004-07-12 EP EP04743948A patent/EP1653966A1/en not_active Withdrawn
- 2004-07-12 WO PCT/IB2004/002286 patent/WO2005007166A1/en active Application Filing
- 2004-07-15 TW TW093121146A patent/TW200505410A/en unknown
Patent Citations (7)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US20030055070A1 (en) * | 1999-07-01 | 2003-03-20 | Wilma Harrison | Phosphodiesterase type 5 (PDE5) inhibitors for the treatment of selective serotonin reuptake inhibitor (SSR) induced sexual dysfunction |
| US20020052370A1 (en) * | 2000-07-06 | 2002-05-02 | Barber Christopher Gordon | Cyclopentyl-substituted glutaramide derivatives as inhibitors of neutral endopeptidase |
| WO2002072586A1 (en) * | 2001-03-09 | 2002-09-19 | Pfizer Limited | Pyrazolo'4,3-d-pyrimidine for inhibiting cgmp pde |
| WO2002074288A2 (en) * | 2001-03-15 | 2002-09-26 | Vernalis Research Limited | Treatment and prevention of sexual dysfunction resulting from ssri-therapy by using a tetrahydrobenz cd indole-6-carboxamide |
| WO2003035072A1 (en) * | 2001-10-20 | 2003-05-01 | Boehringer Ingelheim Pharma Gmbh & Co. Kg | Use of flibanserin in the treatment of sexual disorders |
| US20030104980A1 (en) * | 2001-10-20 | 2003-06-05 | Boehringer Ingelheim Pharma Kg | Treating sexual desire disorders with flibanserin |
| WO2004041259A1 (en) * | 2002-11-06 | 2004-05-21 | Pfizer Limited | Treatment of female sexual dysfunction |
Cited By (66)
| Publication number | Priority date | Publication date | Assignee | Title |
|---|---|---|---|---|
| US10675280B2 (en) | 2001-10-20 | 2020-06-09 | Sprout Pharmaceuticals, Inc. | Treating sexual desire disorders with flibanserin |
| US9782403B2 (en) | 2001-10-20 | 2017-10-10 | Sprout Pharmaceuticals, Inc. | Treating sexual desire disorders with flibanserin |
| US8227471B2 (en) | 2001-10-20 | 2012-07-24 | Sprout Pharmaceuticals, Inc. | Treating sexual desire disorders with flibanserin |
| US11058683B2 (en) | 2001-10-20 | 2021-07-13 | Sprout Pharmaceuticals, Inc. | Treating sexual desire disorders with flibanserin |
| WO2005053697A3 (en) * | 2003-12-01 | 2005-08-18 | Akzo Nobel Nv | Treatment of sexual disorders |
| WO2005053697A2 (en) * | 2003-12-01 | 2005-06-16 | Akzo Nobel N.V. | Treatment of sexual disorders |
| US7538116B2 (en) | 2003-12-01 | 2009-05-26 | Michael Gibertini | Treatment of sexual disorders |
| WO2005102342A1 (en) * | 2004-04-22 | 2005-11-03 | Boehringer Ingelheim International Gmbh | New pharmaceutical compositions for the treatment of sexual disorders ii |
| EP1740180A1 (en) * | 2004-04-22 | 2007-01-10 | Boehringer Ingelheim Pharmaceuticals, Inc. | Use of flibanserin in the treatment of premenstrual and other female sexual disorders |
| AU2005235422B2 (en) * | 2004-04-22 | 2011-08-11 | Boehringer Ingelheim International Gmbh | New pharmaceutical compositions for the treatment of sexual disorders II |
| US9700566B2 (en) | 2004-05-11 | 2017-07-11 | Eb Ip Lybrido B.V. | Pharmaceutical formulations and uses thereof in the treatment of female sexual dysfunction |
| US8227453B2 (en) | 2004-05-11 | 2012-07-24 | Emotional Brain B.V. | Pharmaceutical formulations and uses thereof in the treatment of female sexual dysfunction |
| US9192669B2 (en) | 2004-05-11 | 2015-11-24 | Eb Ip Lybrido B.V. | Pharmaceutical formulations and uses thereof in the treatment of female sexual dysfunction |
| US10441592B2 (en) | 2004-05-11 | 2019-10-15 | Eb Ip Lybrido B.V. | Pharmaceutical formulations and uses thereof in the treatment of female sexual dysfunction |
| US10874668B2 (en) | 2005-08-03 | 2020-12-29 | Sprout Pharmaceuticals, Inc. | Use of Flibanserin in the treatment of obesity |
| US8785458B2 (en) | 2005-08-03 | 2014-07-22 | Sprout Pharmaceuticals, Inc. | Use of flibanserin in the treatment of obesity |
| US10335407B2 (en) | 2005-08-03 | 2019-07-02 | Sprout Pharmaceuticals, Inc. | Use of flibanserin in the treatment of obesity |
| US8227476B2 (en) | 2005-08-03 | 2012-07-24 | Sprout Pharmaceuticals, Inc. | Use of flibanserin in the treatment of obesity |
| US9730927B2 (en) | 2005-08-03 | 2017-08-15 | Sprout Pharmaceuticals, Inc. | Use of flibanserin in the treatment of obesity |
| WO2007048801A2 (en) * | 2005-10-29 | 2007-05-03 | Boehringer Ingelheim International Gmbh | Sexual desire enhancing medicaments comprising benzimidazolone derivatives |
| JP2009513604A (en) * | 2005-10-29 | 2009-04-02 | ベーリンガー インゲルハイム インターナショナル ゲゼルシャフト ミット ベシュレンクテル ハフツング | Benzimidazolone derivatives for the treatment of premenstrual disorders and other female sexual disorders |
| US7923449B2 (en) | 2005-10-29 | 2011-04-12 | Boehringer Ingelheim International Gmbh | Benzimidazolone derivatives for the treatment of premenstrual and other female sexual disorders |
| WO2007048803A1 (en) * | 2005-10-29 | 2007-05-03 | Boehringer Ingelheim International Gmbh | Benzimidazolone derivatives for the treatment of premenstrual and other female sexual disorders |
| WO2007048801A3 (en) * | 2005-10-29 | 2007-06-14 | Boehringer Ingelheim Int | Sexual desire enhancing medicaments comprising benzimidazolone derivatives |
| US9737548B2 (en) | 2005-11-11 | 2017-08-22 | Eb Ip Lybrido B.V. | Pharmaceutical formulations and uses thereof in the treatment of female sexual dysfunction |
| US9333203B2 (en) | 2005-11-11 | 2016-05-10 | Eb Ip Lybrido B.V. | Pharmaceutical formulations and uses thereof in the treatment of female sexual dysfunction |
| JP2013241463A (en) * | 2005-11-11 | 2013-12-05 | Emotional Brain Bv | Pharmaceutical combination comprising testosterone in treatment of female sexual dysfunction |
| WO2007128802A3 (en) * | 2006-05-09 | 2008-06-12 | Boehringer Ingelheim Int | Use of flibanserin for the treatment of post-menopausal sexual desire disorders |
| AU2007247094B2 (en) * | 2006-05-09 | 2012-11-01 | Sprout Pharmaceuticals, Inc. | Use of flibanserin for the treatment of post-menopausal Sexual Desire Disorders |
| WO2007128802A2 (en) * | 2006-05-09 | 2007-11-15 | Boehringer Ingelheim International Gmbh | Use of flibanserin for the treatment of post-menopausal sexual desire disorders |
| JP2009536176A (en) * | 2006-05-09 | 2009-10-08 | ベーリンガー インゲルハイム インターナショナル ゲゼルシャフト ミット ベシュレンクテル ハフツング | Use of flibanserin for the treatment of postmenopausal sexual desire disorders |
| US9763936B2 (en) | 2006-06-30 | 2017-09-19 | Sprout Pharmaceuticals, Inc. | Flibanserin for the treatment of urinary incontinence and related diseases |
| US10004731B2 (en) | 2006-06-30 | 2018-06-26 | Sprout Pharmaceuticals, Inc. | Flibanserin for the treatment of urinary incontinence and related diseases |
| US8545886B2 (en) | 2006-08-14 | 2013-10-01 | Boehringer Ingelheim International Gmbh | Extended release tablet formulations of flibanserin and method for manufacturing the same |
| US8658207B2 (en) | 2006-08-14 | 2014-02-25 | Boehringer Ingelheim International Gmbh | Extended release tablet formulations of flibanserin and method for manufacturing the same |
| US8512748B2 (en) | 2006-08-25 | 2013-08-20 | Boehringer Ingelheim International Gmbh | Controlled release system and method for manufacturing the same |
| AU2007314736B2 (en) * | 2006-11-03 | 2014-01-23 | Eb Ip Lybridos B.V. | Use of 3-alpha-androstanediol, optionally in combination with a 5-HT1A agonist, in the treatment of sexual dysfunction |
| JP2017132809A (en) * | 2006-11-03 | 2017-08-03 | イービー アイピー ライブリドス ビー.ブイ. | Use of testosterone and 5-ht1a agonist for treating sex malfunction |
| CN103599536A (en) * | 2006-11-03 | 2014-02-26 | 情感智能有限责任公司 | Use of 3-alpha-androstanediol in the treatment of sexual dysfunction, optionally in combination with a 5-HT1A agonist |
| US8669242B2 (en) | 2006-11-03 | 2014-03-11 | Emotional Brain B.V. | Use of testosterone and a 5-HT1A agonist in the treatment of sexual dysfunction |
| JP2014111608A (en) * | 2006-11-03 | 2014-06-19 | Emotional Medical Bv | USE OF 3-α-ANDROSTANEDIOL, OPTIONALLY IN COMBINATION WITH 5-HT1A AGONIST, IN TREATMENT OF SEXUAL DYSFUNCTION |
| WO2008054213A2 (en) * | 2006-11-03 | 2008-05-08 | Emotional Brain B.V. | Use of testosterone and a 5-ht1a agonist in the treatment of sexual dysfunction |
| CN104524580A (en) * | 2006-11-03 | 2015-04-22 | 情感智能有限责任公司 | Use of 3-alpha-androstanediol, in combination with a PDE5 inhibitor, in the treatment of sexual dysfunction |
| WO2008054215A2 (en) * | 2006-11-03 | 2008-05-08 | Emotional Brain B.V. | Use of 3-alpha-androstanediol, optionally in combination with a 5-ht1a agonist, in the treatment of sexual dysfunction |
| JP2015157849A (en) * | 2006-11-03 | 2015-09-03 | イービー アイピー ライブリドス ビー.ブイ. | Use of testosterone and 5-ht1a agonist for treating sex malfunction |
| EP2937086A1 (en) * | 2006-11-03 | 2015-10-28 | EB IP Lybridos B.V. | Use of testosterone and a 5-ht1a agonist in the treatment of sexual dysfunction |
| US8648060B2 (en) | 2006-11-03 | 2014-02-11 | Emotional Brain B.V. | Use of 3-alpha-androstanediol in combination with a 5-HT1a agonist, in the treatment of sexual dysfunction |
| US9211334B2 (en) | 2006-11-03 | 2015-12-15 | Eb Ip Lybridos B.V. | Use of testosterone and a 5-HT1A agonist in the treatment of sexual dysfunction |
| AU2007314734B2 (en) * | 2006-11-03 | 2014-01-30 | Eb Ip Lybridos B.V. | Use of testosterone and a 5-HT1A agonist in the treatment of sexual dysfunction |
| US9597335B2 (en) | 2006-11-03 | 2017-03-21 | Eb Ip Lybridos B.V. | Use of testosterone and a 5-HT1A agonist in the treatment of sexual dysfunction |
| JP2014001235A (en) * | 2006-11-03 | 2014-01-09 | Emotional Medical Bv | Use of testosterone and 5-ht1a agonist for treating sex malfunction |
| US8653051B2 (en) | 2006-11-03 | 2014-02-18 | Emotional Brain B.V. | Use of 3-alpha-androstanediol in combination with a PDE5 inhibitor, in the treatment of sexual dysfunction |
| CN103381270A (en) * | 2006-11-03 | 2013-11-06 | 情感智能有限责任公司 | Use of testosterone and a 5-ht1a agonist in the treatment of sexual dysfunction |
| US8575139B2 (en) | 2006-11-03 | 2013-11-05 | Emotional Brain B.V. | Use of testosterone and a 5-HT1a agonist in the treatment of sexual dysfunction |
| RU2463054C2 (en) * | 2006-11-03 | 2012-10-10 | Эмоушнл Брэйн Б.В. | Use of testosterone and 5-ht1a agonist for treating sexual dysfunction |
| JP2010509213A (en) * | 2006-11-03 | 2010-03-25 | エモーショナル ブレイン ビー.ブイ. | Use of 3-α-androstanediol, optionally in combination with a 5-HT1a agonist, in the treatment of sexual dysfunction |
| RU2646447C2 (en) * | 2006-11-03 | 2018-03-05 | ЭБ ИП Либридос Б.В. | Use of testosterone analogue and 5-ht1a agonist for sexual dysfunction treatment |
| JP2010509211A (en) * | 2006-11-03 | 2010-03-25 | エモーショナル ブレイン ビー.ブイ. | Use of testosterone and 5-HT1A agonists in the treatment of sexual dysfunction |
| EP1925307A1 (en) * | 2006-11-03 | 2008-05-28 | Emotional Brain B.V. | Use of 3-alpha-androstanediol in the treatment of sexual dysfunction |
| NO343597B1 (en) * | 2006-11-03 | 2019-04-08 | Eb Ip Lybridos B V | Use of testosterone and a 5-HT1A agonist in the treatment of sexual dysfunction |
| US10314848B2 (en) | 2006-11-03 | 2019-06-11 | Eb Ip Lybridos B.V. | Use of testosterone and a 5-HT1A agonist in the treatment of sexual dysfunction |
| WO2008054213A3 (en) * | 2006-11-03 | 2009-04-09 | Emotional Brain Bv | Use of testosterone and a 5-ht1a agonist in the treatment of sexual dysfunction |
| WO2008054215A3 (en) * | 2006-11-03 | 2009-04-09 | Emotional Brain Bv | Use of 3-alpha-androstanediol, optionally in combination with a 5-ht1a agonist, in the treatment of sexual dysfunction |
| EP2896624A1 (en) | 2007-03-28 | 2015-07-22 | Atir Holding S.A. | Heterotricyclic compounds as serotonergic and/or dopaminergic agents and uses thereof |
| US10166230B2 (en) | 2007-09-12 | 2019-01-01 | Sprout Pharmaceuticals Inc. | Treatment of vasomotor symptoms |
| EP2695932A1 (en) | 2012-08-08 | 2014-02-12 | Ab Nanol Technologies Oy | Grease composition |
Also Published As
| Publication number | Publication date |
|---|---|
| EP1653966A1 (en) | 2006-05-10 |
| TW200505410A (en) | 2005-02-16 |
| JP2007516949A (en) | 2007-06-28 |
| MXPA06000623A (en) | 2006-04-11 |
| CA2532252A1 (en) | 2005-01-27 |
| BRPI0411985A (en) | 2006-08-29 |
Similar Documents
| Publication | Publication Date | Title |
|---|---|---|
| US20050065158A1 (en) | Treatment of sexual dysfunction | |
| EP1653966A1 (en) | Treatment of sexual dysfunction | |
| US20080153841A1 (en) | Treatment of premature ejaculation | |
| US20020165237A1 (en) | Treatment of the insulin resistance syndrome | |
| KR20030023747A (en) | Treatment of the insulin resistance syndrome | |
| EP1149579A2 (en) | Use of an estrogen agonist/antagonist for treating female sexual dysfunction | |
| EP1355651A2 (en) | Treatment of diabetes mellitus using vardenafil | |
| US20040029891A1 (en) | Use of PDE5 inhibitors in the treatment of polycystic ovary syndrome | |
| KR20080084943A (en) | Pharmaceutical formulations and uses thereof in the treatment of female sexual dysfunction | |
| AU2018310881A1 (en) | Use of mavoglurant in the reduction of cocaine use or in preventing relapse into cocaine use | |
| US20030055070A1 (en) | Phosphodiesterase type 5 (PDE5) inhibitors for the treatment of selective serotonin reuptake inhibitor (SSR) induced sexual dysfunction | |
| EP1335730B1 (en) | Use of pde5 inhibitors for the treatment of premature ejaculation | |
| ZA200409532B (en) | Novel combination | |
| AU2002215149A1 (en) | Treatment of premature ejaculation | |
| US20050148585A1 (en) | Treatment of wounds | |
| CA2415791A1 (en) | Treatment of wounds | |
| WO2023135505A1 (en) | Tlr7/8-antagonist for treating sjögren's syndrome or mixed connective tissue disease |
Legal Events
| Date | Code | Title | Description |
|---|---|---|---|
| AK | Designated states |
Kind code of ref document: A1 Designated state(s): AE AG AL AM AT AU AZ BA BB BG BR BW BY BZ CA CH CN CO CR CU CZ DE DK DM DZ EC EE EG ES FI GB GD GE GH GM HR HU ID IL IN IS JP KE KG KP KR KZ LC LK LR LS LT LU LV MA MD MG MK MN MW MX MZ NA NI NO NZ OM PG PH PL PT RO RU SC SD SE SG SK SL SY TJ TM TN TR TT TZ UA UG US UZ VC VN YU ZA ZM ZW |
|
| AL | Designated countries for regional patents |
Kind code of ref document: A1 Designated state(s): GM KE LS MW MZ NA SD SL SZ TZ UG ZM ZW AM AZ BY KG KZ MD RU TJ TM AT BE BG CH CY CZ DE DK EE ES FI FR GB GR HU IE IT LU MC NL PL PT RO SE SI SK TR BF BJ CF CG CI CM GA GN GQ GW ML MR NE SN TD TG |
|
| WWE | Wipo information: entry into national phase |
Ref document number: 2004743948 Country of ref document: EP |
|
| DPEN | Request for preliminary examination filed prior to expiration of 19th month from priority date (pct application filed from 20040101) | ||
| 121 | Ep: the epo has been informed by wipo that ep was designated in this application | ||
| ENP | Entry into the national phase |
Ref document number: 2532252 Country of ref document: CA |
|
| WWE | Wipo information: entry into national phase |
Ref document number: PA/a/2006/000623 Country of ref document: MX Ref document number: 2006520035 Country of ref document: JP |
|
| WWP | Wipo information: published in national office |
Ref document number: 2004743948 Country of ref document: EP |
|
| ENP | Entry into the national phase |
Ref document number: PI0411985 Country of ref document: BR |