
Risk Factors Associated with CIN2+ in Spanish Patients with L-SIL/ASCUS Cytology Collected from a Madrid Hospital
 and
and
Abstract
:1. Introduction
2. Material and Methods
Statistical Analysis
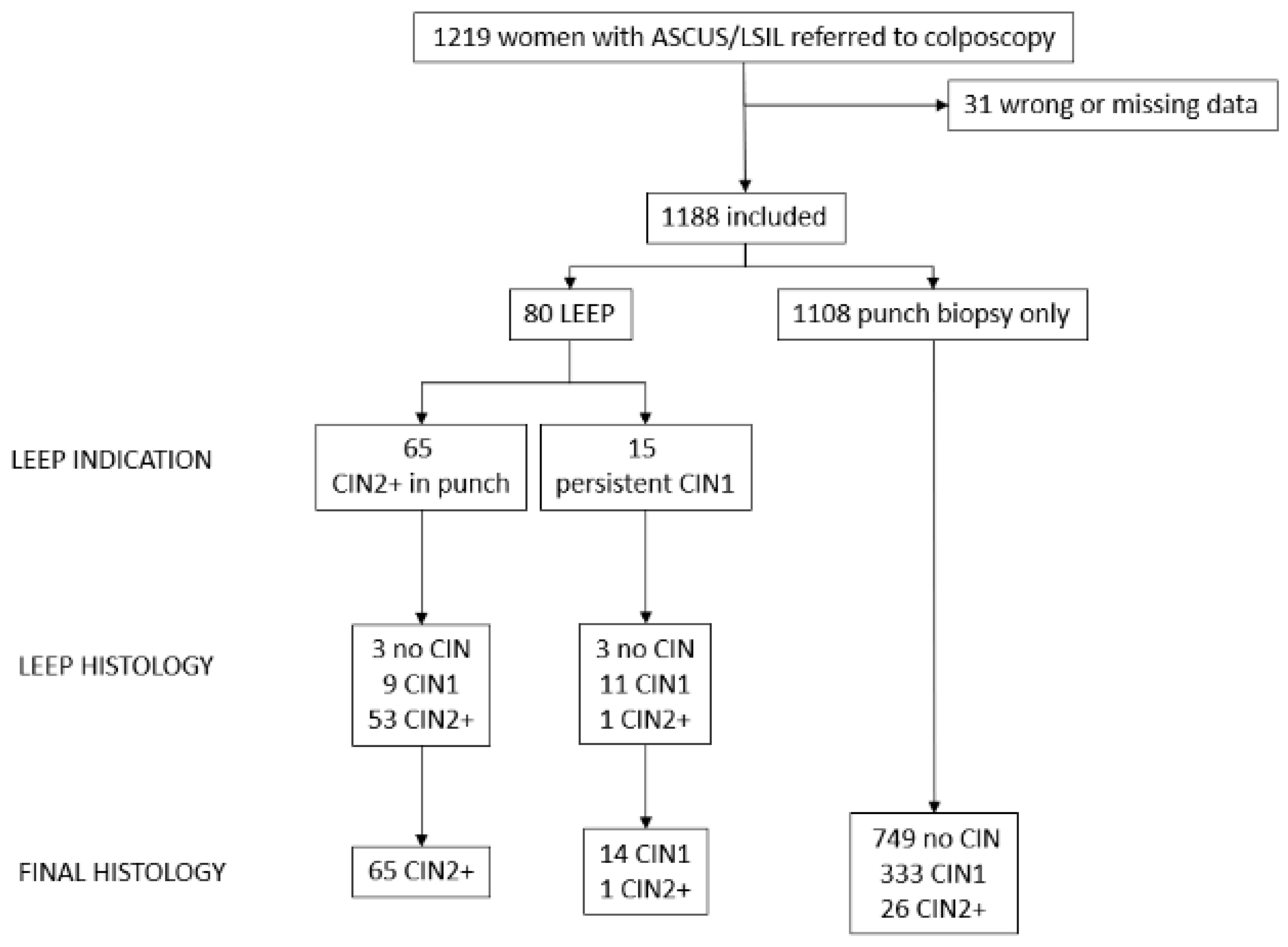
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GLOBOCAN 2020. Map Production: IARC. World Health Organization. Available online: http://gco.iarc.fr/today (accessed on 15 November 2022).
- Arbyn, M.; Ronco, G.; Anttila, A.; Meijer, C.J.; Poljak, M.; Ogilvie, G.; Koliopoulos, G.; Naucler, P.; Sankaranarayanan, R.; Peto, J. Evidence regarding human papillomavirus testing in secondary prevention of cervical cancer. Vaccine 2012, 30 (Suppl. S5), F88–F99. [Google Scholar] [CrossRef] [PubMed]
- Torné, A.; Andía, D.; Castro, M.; de la Fuente, J.; Hernández, J.J.; López, J.A.; Martínez, J.C.; Medina, N.; Quílez, J.C.; Ramírez Mena, M.; et al. AEPCC-Guía: Colposcopia. Estándares de Calidad; Publicaciones AEPCC: Madrid, Spain, 2018; pp. 1–80. [Google Scholar]
- OMS. Control Integral del Cáncer Cervicouterino. Guía de Prácticas Esenciales, 2nd ed.; OPS: Washington, DC, USA, 2016. [Google Scholar]
- Schiffman, M.; Solomon, D. Findings to date from the ASCUS-LSIL Triage Study (ALTS). Arch. Pathol. Lab. Med. 2003, 127, 946–949. [Google Scholar] [CrossRef]
- Torné, A.; Andía, D.; Bruni, L.; Centeno, C.; Coronado, P.; Cruz Quílez, J.; de la Fuente, J.; de Sanjosé, S.; Granados, R.; Ibáñez, R.; et al. AEPCC-Guía: Prevención Secundaria del Cáncer de Cuello del Útero. Conducta Clínica Ante Resultados Anormales de las Pruebas de Cribado; AEPCC: Madrid, Spain, 2022. [Google Scholar]
- Cortés, J.; Martinón-Torres, F.; Ramón y Cajal, J.M.; Gil, Á.; Velasco, J.; Abizanda, M.; Miranda, P.; Garrido, R. Prevención primaria y secundaria de los cánceres de cuello de útero y vulva: Recomendaciones para la práctica clínica. Prog. Obstet. Ginecol. 2010, 53 (Suppl. S1), 1–19. [Google Scholar]
- AEPCC-Guía: Prevención del Cáncer de Cuello de Útero; Publicaciones AEPC: Madrid, Spain, 2015.
- Coronado, P.J.; Fasero, M. Colposcopy combined with dynamic spectral imaging. A prospective clinical study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 196, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Coronado, P.J.; González, V.; Fasero, M. Value of colposcopy with dynamic spectral imaging in the detection and evolution of high-grade cervical lesions. Expert Rev. Med. Devices 2022, 19, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Tatti, S.; Bornstein, J.; Prendiville, W. Colposcopy: A global perspective: Introduction of the new IFCPC colposcopy terminology. Obstet. Gynecol. Clin. N. Am. 2013, 40, 235–250. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, J.; Bentley, J.; Bösze, P.; Girardi, F.; Haefner, H.; Menton, M.; Perrotta, M.; Prendiville, W.; Russell, P.; Sideri, M.; et al. 2011 colposcopic terminology of the International Federation for Cervical Pathology and Colposcopy. Obstet Gynecol. 2012, 120, 166–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charlton, B.M.; Carwile, J.L.; Michels, K.B.; Feldman, S. A cervical abnormality risk prediction model: Can we use clinical information to predict which patients with ASCUS/LSIL Pap tests will develop CIN 2/3 or AIS? J. Low. Genit. Tract Dis. 2013, 17, 242–247. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.S.; Zuna, R.E.; Wentzensen, N.; Dunn, S.T.; Sherman, M.E.; Gold, M.A.; Schiffman, M.; Wacholder, S.; Allen, R.A.; Block, I.; et al. Human papillomavirus cofactors by disease progression and human papillomavirus types in the study to understand cervical cancer early endpoints and determinants. Cancer Epidemiol. Biomark. Prev. 2009, 18, 113–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, L.C.; Egemen, D.; Chen, X.; Katki, H.A.; Demarco, M.; Wiser, A.L.; Perkins, R.B.; Guido, R.S.; Wentzensen, N.; Schiffman, M. 2019 ASCCP Risk-Based Management Consensus Guidelines: Methods for Risk Estimation, Recommended Management, and Validation. J. Low. Genit. Tract Dis. 2020, 24, 90–101. [Google Scholar] [CrossRef]
- Demarco, M.; Lorey, T.S.; Fetterman, B.; Cheung, L.C.; Guido, R.S.; Wentzensen, N.; Kinney, W.K.; Poitras, N.E.; Befano, B.; Castle, P.E.; et al. Risks of CIN 2+, CIN 3+, and Cancer by Cytology and Human Papillomavirus Status: The Foundation of Risk-Based Cervical Screening Guidelines. J. Low. Genit. Tract Dis. 2017, 21, 261–267. [Google Scholar] [CrossRef]
- McIntyre-Seltman, K.; Castle, P.E.; Guido, R.; Schiffman, M.; Wheeler, C.M.; ALTS Group. Smoking is a risk factor for cervical intraepithelial neoplasia grade 3 among oncogenic human papillomavirus DNA-positive women with equivocal or mildly abnormal cytology. Cancer Epidemiol. Biomark. Prev. 2005, 14, 1165–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demarco, M.; Egemen, D.; Raine-Bennett, T.R.; Cheung, L.C.; Befano, B.; Poitras, N.E.; Lorey, T.S.; Chen, X.; Gage, J.C.; Castle, P.E.; et al. A Study of Partial Human Papillomavirus Genotyping in Support of the 2019 ASCCP Risk-Based Management Consensus Guidelines. J. Low. Genit. Tract Dis. 2020, 24, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Dorji, N.; Tshering, S.; Choden, S.; Chhetri, M.; Bhujel, D.; Wangden, T.; Pradhan, B.; Bhutia, P.C.; Tshomo, U. Evaluation of the diagnostic performance of colposcopy in the diagnosis of histologic cervical intraepithelial neoplasia 2+ (CIN2+). BMC Cancer 2022, 22, 930. [Google Scholar] [CrossRef]


{kind=link}
| N (%)/Mean (SD) N = 1188 | |
|---|---|
| Age (years) | 35.2 (10.4) |
| Age at first sexual intercourse | 17.2 (5.3) |
| Number of sexual partners | 7.3 (8.6) |
| Anal sexual intercourse | 199 (16.8%) |
| Current Smoker | 154 (12.9%) |
| Pap-smear | |
| ASCUS | 472 (39.7%) |
| L-SIL | 706 (59.4%) |
| CC/C-DSI result | |
| Normal/Metaplasia | 458 (38.6%) |
| Changes grade 1 | 626 (52.7%) |
| Changes grade 2 | 93 (7.8%) |
| Cancer | 1 (0.0%) |
| HPV | |
| Genotype 16/18 | 152 (12.8%) |
| High-risk HPV No. 16/18 | 282 (23.8%) |
| Low-risk HPV | 124 (10.4%) |
| Negative | 181 (15.2%) |
| Undetermined | 439 (37.0%) |
| Inmunocompromise | |
| HIV | 11 (0.9%) |
| Other | 29 (2.4%) |
| Patients who required LEEP | 90 (7.6%) |
| Normal/Changes grade 1 | 32 (2.7%) |
| Changes grade 2 | 58 (4.9%) |
| OR (IC 95%) | p | |
|---|---|---|
| Age | 0.8 (−1.1–2.7) * | 0.4 |
| HR-HPV | 2.1 (1.4–3.2) | <0.001 |
| HVP 16/18 | 12.7 (5.5–29.4) | <0.001 |
| HR-HPV No. 16/18 | 3.1 /1.3–7.4) | 0.01 |
| ≥5 sexual partners | 1.4 (0.9–2.3) | 0.12 |
| Anal intercourse | 1.6 (1–2.5) | 0.08 |
| Current smoker | 2.2 (1.4–3.5) | <0.001 |
| DSI + CC | 0.6 (0.37–0.83) | <0.05 |
| Smoking + HR-VPH | 2.9 (1.7–5.0) | <0.001 |
| HPV Vaccine | 0.8 (0.4–1.5) | 0.5 |
| Postmenopausal status | 0.4 (1.2–1.3) | 0.1 |
| Immunocompromise | 1.8 (0.8–4.3) | 0.2 |
| HIV | 1.9 (0.3–8.8) | 0.33 |
| OR (IC 95%) | p | |
|---|---|---|
| HVP 16/18 | 12.7 (3.6–44.9) | <0.001 |
| HR-HPV No. 16/18 | 3.1 (0.9–11.4) | 0.08 |
| Anal intercourse | 0.5 (0.3–1.0) | 0.08 |
| Current smoker | 0.2 (0.1–1.1) | 0.06 |
| DSI + CC | 0.6 (0.4–0.9) | 0.03 |
| Smoking + HR-HPV | 3.1 (0.6–17.1) | 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González González, V.; Ramírez Mena, M.; Herráiz Martínez, M.Á.; Serrano García, I.; Coronado Martín, P.J. Risk Factors Associated with CIN2+ in Spanish Patients with L-SIL/ASCUS Cytology Collected from a Madrid Hospital. J. Pers. Med. 2022, 12, 1944. https://doi.org/10.3390/jpm12121944
González González V, Ramírez Mena M, Herráiz Martínez MÁ, Serrano García I, Coronado Martín PJ. Risk Factors Associated with CIN2+ in Spanish Patients with L-SIL/ASCUS Cytology Collected from a Madrid Hospital. Journal of Personalized Medicine. 2022; 12(12):1944. https://doi.org/10.3390/jpm12121944
Chicago/Turabian StyleGonzález González, Virginia, Mar Ramírez Mena, Miguel Ángel Herráiz Martínez, Irene Serrano García, and Pluvio J. Coronado Martín. 2022. "Risk Factors Associated with CIN2+ in Spanish Patients with L-SIL/ASCUS Cytology Collected from a Madrid Hospital" Journal of Personalized Medicine 12, no. 12: 1944. https://doi.org/10.3390/jpm12121944